

COVID-19, broad-spectrum therapeutics and the magic blanket paradigm
Posted: 12 April 2021 | Dr Praveen Prathapan (Research Consultant) | No comments yet
Dr Praveen Prathapan explains why broad-spectrum therapeutics need to be identified to provide a safety net against pandemics, including COVID-19.

The pandemic has challenged the paradigm of drug development. Over a century ago, Paul Ehrlich’s magic bullet, a hypothetical drug that targets a given pathogen without harming the host, materialised in the 20th century as a plethora of therapeutics successfully treating diseases around the world.1,2 When COVID-19 emerged there were, however, no magic bullets.3,4 A year since the pandemic began, there are still over 300 therapeutic candidates being developed in various stages of pre-clinical or clinical research, making evident that de novo magic bullets for novel pandemics can only be developed after a pandemic has emerged.
With regular news updates and feature articles, our COVID-19 hub has everything you need to keep up to date with R&D during the pandemic. Click below to visit:
In 2007, in their Strategic Plan for Biodefense Research, the US Department of Health and Human Services described the need for special drugs that can kill any pathogen in order to prepare for pandemics and bioterrorist threats.5,6 Contrary to magic bullets, which must be developed after a pandemic emerges, these ‘magic blankets’ can be developed in anticipation of infectious threats and be used against a myriad of pathogen types.
Unfortunately, no such drugs were formally discovered and the SARS-CoV-2 pandemic led to a furore of potential emergency treatments propounded against the novel disease. The most infamous of these, hydroxychloroquine, was an antiparasitic drug. Indeed, there is evidence of not just hydroxychloroquine, but a myriad of antiparasitic and indeed antibiotic drugs that display antiviral activity.7
Drug Target Review has just announced the launch of its NEW and EXCLUSIVE report examining the evolution of AI and informatics in drug discovery and development.
In this 63 page in-depth report, experts and researchers explore the key benefits of AI and informatics processes, reveal where the challenges lie for the implementation of AI and how they see the use of these technologies streamlining workflows in the future.
Also featured are exclusive interviews with leading scientists from AstraZeneca, Auransa, PolarisQB and Chalmers University of Technology.
To discern how antiviral a given antibiotic or antiparasitic drug is, we used the Drug Repositioning Evidence Level (DREL) system propounded by Opera and Overington in their seminal review of drug repositioning studies.8 An advantage of this particular system is its parallelism with classification schemes used for quantifying drug-drug interactions. As quality of evidence increases from in vitro investigations to animal and human clinical trials, a higher DREL number is assigned accordingly (Figure 1). The DREL assessment was borne out of unsubstantiated claims for repositioning projects and a lack of experimental evidence or corroboration with the literature. As a measure of the pharmacological and clinical evidence of given drug against a particular disease, the DREL system provided us with a simple yet useful method of comparing the potential efficacy of any drug against COVID-19.
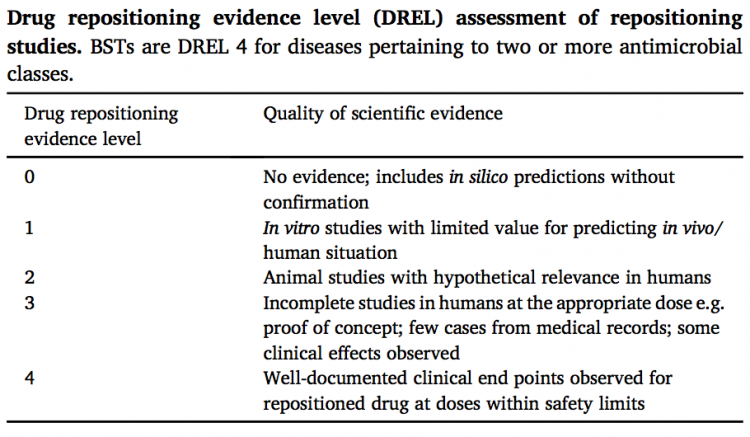
Figure 1
When we did this, however, we discovered something startling. At least two of the drugs being trialled against COVID-19 were DREL 4 for more than one pathogen type (that is, clinically and pharmacologically effective against infection by more than one pathogen type): azithromycin, a macrolide antibiotic that is used to treat malaria; and nitazoxanide, a broad-spectrum antiparasitic and antiviral agent that is effective against bacterial infections.9
To our knowledge, these drugs represent the first of a new antimicrobial class, a class that recognises drugs that are effective against multiple infection types. In our review of azithromycin entitled Azithromycin: The First Broad-spectrum Therapeutic, we coined the term ‘broad-spectrum therapeutic’ (BST) to describe this new drug class.10 This term reflects both the broad pharmacological profile of these drugs as well as their wide-ranging applicability against different disease types. Using the DREL system, BSTs can be defined alternatively as DREL 4 for multiple diseases pertaining to more than one pathogen class. A BST that is used clinically as an antimalarial and an antiviral but has not been studied as an antibiotic or antifungal is a 0:0:4:4 BST; the order of the DREL numbers here are: antibiotic = 0, antifungal = 0, antiparasitic = 4, antiviral = 4. According to this system, azithromycin is a 4:0:4:2 BST and nitazoxanide a 4:0:4:4 BST.
 As the discovery of antibiotics has advanced our understanding of bacterial infection over the last century, so the discovery of BSTs will unearth infection mechanisms conserved across pathogen classes. Indeed, azithromycin’s lysosomotropic properties have shown to be useful against both malarial and viral infections. Furthermore, identification of cellular and nuclear signalling pathways targeted by BSTs, such as azithromycin’s modulation of antiviral responses via IFNβ activation and nitazoxanide’s inhibition of autophagy via ING1 upregulation, will instigate and iteratively improve BST drug-disease interaction networks, further contributing to a shift away from the ‘single drug-single target’ paradigm and towards a polypharmacological one in which therapeutics engage multiple targets within the interactome. This emergence of network pharmacology has already been described as a paradigm shift in medicine.11
As the discovery of antibiotics has advanced our understanding of bacterial infection over the last century, so the discovery of BSTs will unearth infection mechanisms conserved across pathogen classes. Indeed, azithromycin’s lysosomotropic properties have shown to be useful against both malarial and viral infections. Furthermore, identification of cellular and nuclear signalling pathways targeted by BSTs, such as azithromycin’s modulation of antiviral responses via IFNβ activation and nitazoxanide’s inhibition of autophagy via ING1 upregulation, will instigate and iteratively improve BST drug-disease interaction networks, further contributing to a shift away from the ‘single drug-single target’ paradigm and towards a polypharmacological one in which therapeutics engage multiple targets within the interactome. This emergence of network pharmacology has already been described as a paradigm shift in medicine.11
Azithromycin and nitazoxanide are not magic blankets, but they are almost so. With an increasing number of repositioning studies conducted worldwide, particularly with the onset of the COVID-19 pandemic, it is foreseeable that new BSTs will be identified. We point to ivermectin and niclosamide as potential broad-spectrum therapeutics in the near future.12,13 An increasing armamentarium of these novel drugs will enable the identification of conserved chemical and pharmacological properties, which in turn will facilitate the longer-term development of a pipeline for de novo BSTs. Soon, BSTs such as azithromycin can be replaced with more powerful 4:4:4:4 BSTs to prepare for infectious threats, formalising the shift to the magic blanket paradigm first envisioned by the US Department of Health and Human Services 14 years ago.
About the author
Dr Praveen Prathapan is a former researcher at the Department of Biochemistry, University of Oxford and is now a research consultant in London, UK.
References
- Valent P, Groner B, Schumacher U, Superti-Furga G, Busslinger M, Kralovics R, Zielinski C, Penninger JM, Kerjaschki D, Stingl G, Smolen JS, Valenta R, Lassmann H, Kovar H, Jäger U, Kornek G, Müller M, Sörgel F. Paul Ehrlich (1854-1915) and His Contributions to the Foundation and Birth of Translational Medicine. J Innate Immun. 2016;8(2):111-20. doi: 10.1159/000443526. Epub 2016 Feb 5. PMID: 26845587; PMCID: PMC6738855.
- Strebhardt K, Ullrich A. Paul Ehrlich’s magic bullet concept: 100 years of progress. Nat Rev Cancer. 2008 Jun;8(6):473-80. doi: 10.1038/nrc2394. Epub 2008 May 12. PMID: 18469827.
- Kouznetsov VV. COVID-19 treatment: Much research and testing, but far, few magic bullets against SARS-CoV-2 coronavirus. Eur J Med Chem. 2020 Oct 1;203:112647. doi: 10.1016/j.ejmech.2020.112647. Epub 2020 Jul 15. PMID: 32693298; PMCID: PMC7362854.
- Allegrante JP, Auld ME, Natarajan S. Preventing COVID-19 and Its Sequela: “There Is No Magic Bullet… It’s Just Behaviors”. Am J Prev Med. 2020 Aug;59(2):288-292. doi: 10.1016/j.amepre.2020.05.004. Epub 2020 May 30. PMID: 32591282; PMCID: PMC7260531.
- Biodefense Strategic Plan, 2002. NIH: National Institute of Allergy and Infectious Diseases. www.niaid.nih.gov.
- Biodefense Strategic Plan, 2007. NIH: National Institute of Allergy and Infectious Diseases. www.niaid.nih.gov.
- Harrison, C., 2020 Apr. Coronavirus puts drug repurposing on the fast track. Nat. Biotechnol. 38 (4), 379–381. https://doi.org/10.1038/d41587-020-00003-1.
- Oprea, Tudor I., Overington, John P., 2015. Computational and practical aspects of drug repositioning. Assay Drug Dev. Technol. 13 (6), 299–306. https://doi.org/10.1089/ adt.2015.29011.tiodrrr.
- Firth A., Prathapan, P., 2021. Broad-spectrum therapeutics: a new antimicrobial class. Curr. Res. Phar. Drug Disc. 2: 100011. https://doi:10.1016/j.crphar.2020.100011.
- Firth, A., Prathapan, P., 2020. Azithromycin: the first broad-spectrum therapeutic. Eur. J. Med. Chem. 207, 112739. https://doi.org/10.1016/j.ejmech.2020.112739.
- Hopkins AL. Network pharmacology: the next paradigm in drug discovery. Nat Chem Biol. 2008 Nov;4(11):682-90. doi: 10.1038/nchembio.118. PMID: 18936753.
- Crump, A. Ivermectin: enigmatic multifaceted ‘wonder’ drug continues to surprise and exceed expectations. J Antibiot70, 495–505 (2017). https://doi.org/10.1038/ja.2017.11.
- Xu J, Shi PY, Li H, Zhou J. Broad Spectrum Antiviral Agent Niclosamide and Its Therapeutic Potential. ACS Infect Dis. 2020 May 8;6(5):909-915. doi: 10.1021/acsinfecdis.0c00052. Epub 2020 Mar 10. PMID: 32125140; PMCID: PMC7098069.
Related topics
Antibiotics, Drug Development, Drug Leads, Drug repurposing, Therapeutics
Related conditions
Covid-19
Related organisations
US Department of Health and Human Services
Related people
Paul Ehrlich